
HBM4EU Chromates Study—Genotoxicity and Oxidative Stress Biomarkers in Workers Exposed to Hexavalent Chromium

 , , , , , ,
, , , , , ,  , , , , , , , , and add
Show full author list
, , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Workplace and Study Population
2.2. Biological Samples Collection and Biomarkers Analyses
2.3. Cytokinesis-Blocked Micronucleus (CBMN) Assay in Lymphocytes
2.4. Micronucleus (MN) Assay in Reticulocytes (RET)
2.5. Comet Assay
2.6. Oxidative Stress Biomarkers
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
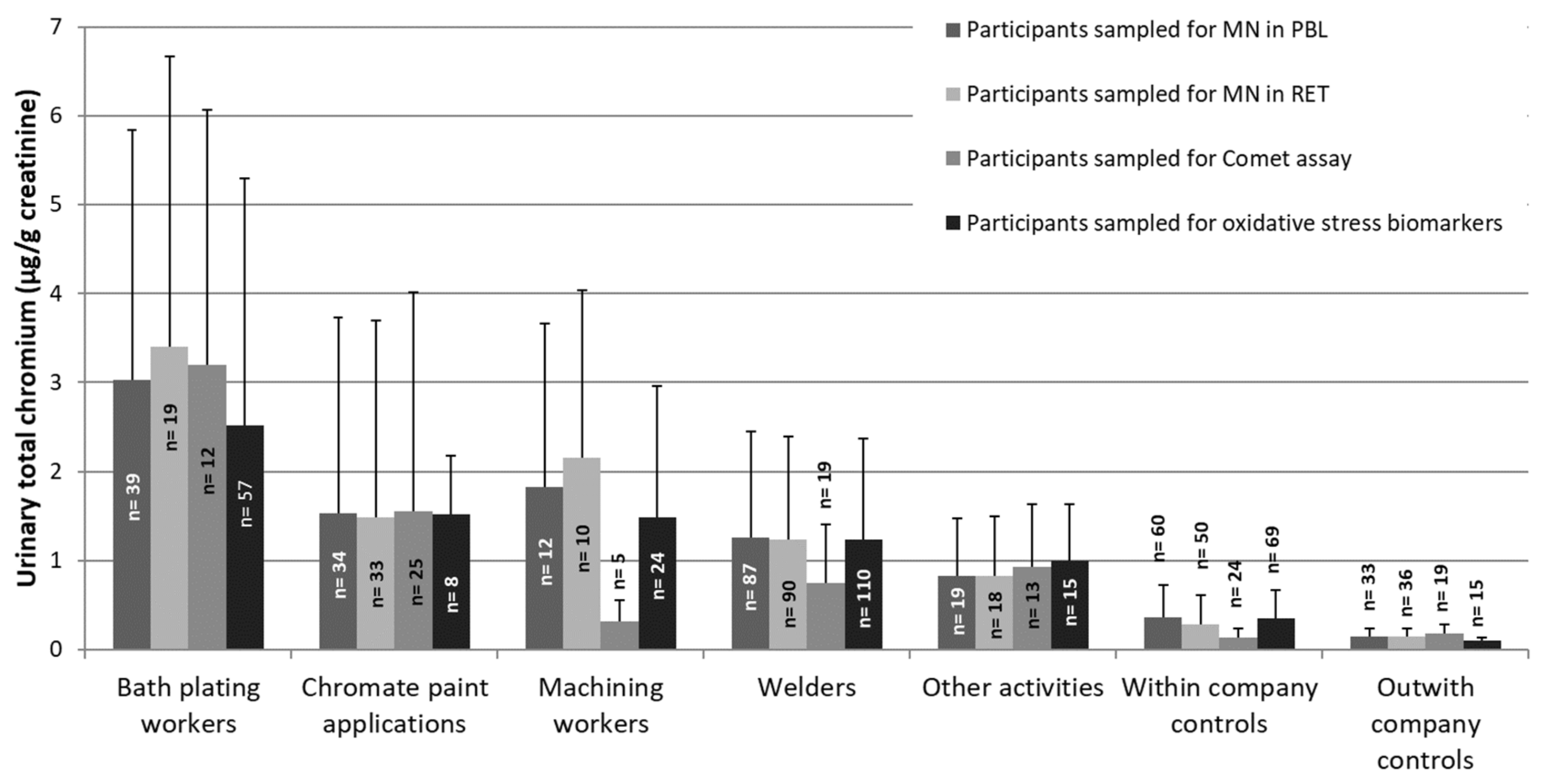
3.2. Activities at the Workplace and Exposure to Cr(VI)
3.3. Genotoxicity Biomarkers in Blood Cells
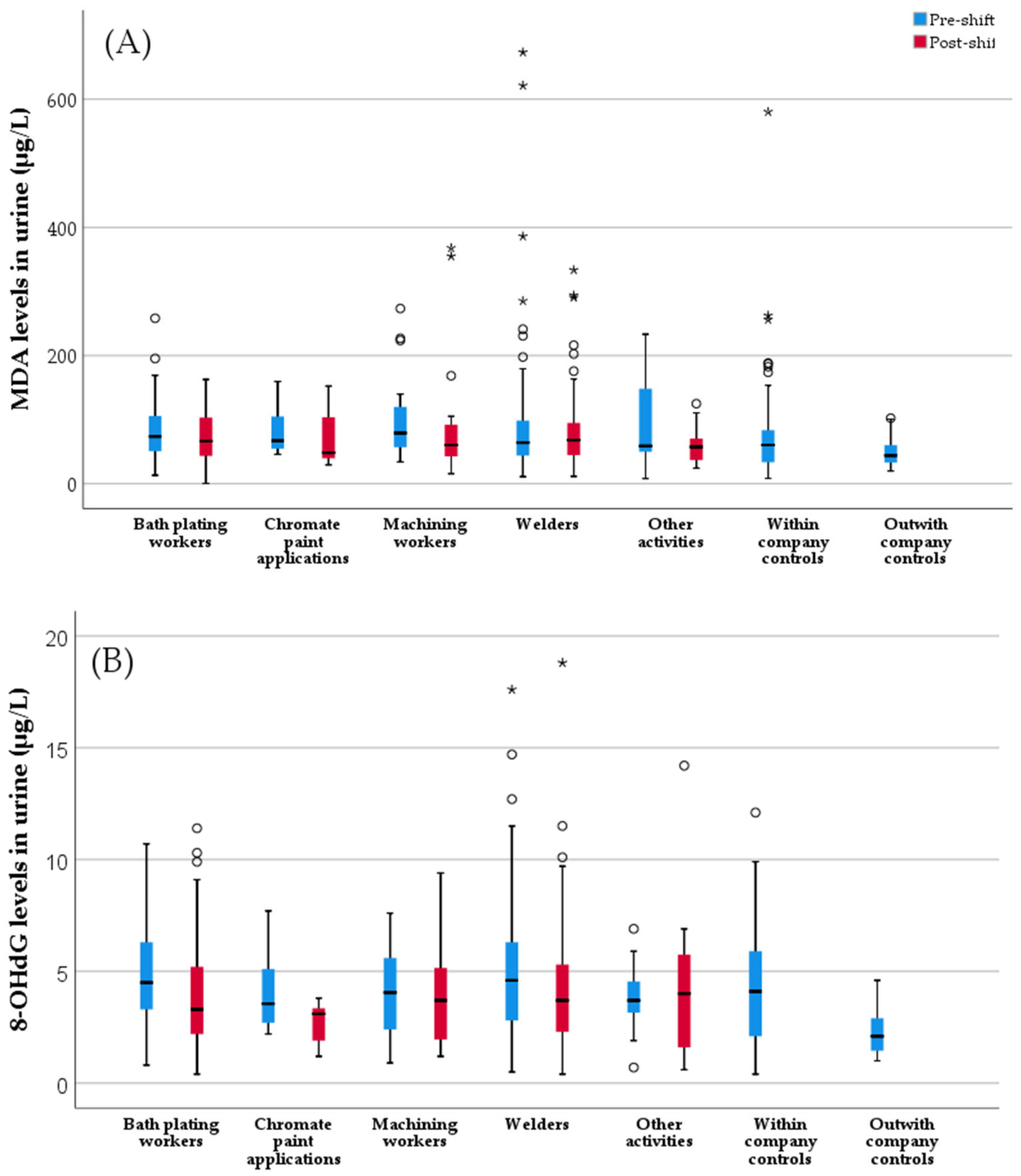
3.4. Oxidative Stress Biomarkers in Urine
3.5. Effects of Predictor Variables on Genotoxicity and Oxidative Stress Biomarkers
3.6. Correlation between Effect Biomarkers
3.7. Correlation between Effect and Exposure Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Annangi, B.; Bonassi, S.; Marcos, R.; Hernández, A. Biomonitoring of humans exposed to arsenic, chromium, nickel, vanadium, and complex mixtures of metals by using the micronucleus test in lymphocytes. Mutat. Res.-Rev. Mutat. Res. 2016, 770, 140–161. [Google Scholar] [CrossRef] [PubMed]
- SCOEL/REC/386 Chromiun VI compounds. In Recommendation from the Scientific Committee on Occupational Exposure Limits; European Commission: Brussels, Belgium, 2017. [CrossRef]
- IARC. Chromium (VI) compounds. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARCPress: Lyon, France, 2018; pp. 147–167. [Google Scholar]
- IARC. Chemical agents and related occupations. In IARC IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARCPress: Lyon, France, 2012; Volume 100, pp. 9–562. [Google Scholar]
- Ventura, C.; Gomes, B.C.; Oberemm, A.; Louro, H.; Huuskonen, P.; Mustieles, V.; Fernández, M.F.; Ndaw, S.; Mengelers, M.; Luijten, M.; et al. Biomarkers of effect as determined in human biomonitoring studies on hexavalent chromium and cadmium in the period 2008–2020. Environ. Res. 2021, 197, 110998. [Google Scholar] [CrossRef]
- Alvarez, C.C.; Bravo Gómez, M.E.; Hernández Zavala, A. Hexavalent chromium: Regulation and health effects. J. Trace Elem. Med. Biol. 2021, 65, 126729. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Guo, Y.; Tsai, P.; Su, L. Use of Inhalable Cr +6 Exposures to Characterize Urinary Chromium Concentrations in Plating Industry Workers. J. Occup. Health 2002, 44, 46–52. [Google Scholar] [CrossRef]
- Viegas, S.; Jeddi, M.Z.; Hopf, N.B.; Bessems, J.; Palmen, N.; Galea, K.S.; Jones, K.; Kujath, P.; Duca, R.-C.; Verhagen, H.; et al. Biomonitoring as an underused exposure assessment tool in occupational safety and health context—Challenges and way forward. Int. J. Environ. Res. Public Health 2020, 17, 5884. [Google Scholar] [CrossRef]
- Navin, A.K.; Aruldhas, M.M. Hexavalent Chromium and Male Reproduction: An Update. Proc. Zool. Soc. 2021, 74, 617–633. [Google Scholar] [CrossRef]
- Hessel, E.V.S.; Staal, Y.C.M.; Piersma, A.H.; den Braver-Sewradj, S.P.; Ezendam, J. Occupational exposure to hexavalent chromium. Part I. Hazard assessment of non-cancer health effects. Regul. Toxicol. Pharmacol. 2021, 126, 105048. [Google Scholar] [CrossRef] [PubMed]
- CDC/NIOSH. Occupational exposure to hexavalent chromium. Final Rule Fed. Regist. 2013, 71, 10099–10385. [Google Scholar]
- Den Braver-Sewradj, S.P.; van Benthem, J.; Staal, Y.C.M.; Ezendam, J.; Piersma, A.H.; Hessel, E.V.S. Occupational exposure to hexavalent chromium. Part II. Hazard assessment of carcinogenic effects. Regul. Toxicol. Pharmacol. 2021, 126, 105045. [Google Scholar] [CrossRef]
- Proctor, D.M.; Suh, M.; Campleman, S.L.; Thompson, C.M. Assessment of the mode of action for hexavalent chromium-induced lung cancer following inhalation exposures. Toxicology 2014, 325, 160–179. [Google Scholar] [CrossRef]
- Nasirzadeh, N.; Mohammadian, Y.; Dehgan, G. Health Risk Assessment of Occupational Exposure to Hexavalent Chromium in Iranian Workplaces: A Meta-analysis Study. Biol. Trace Elem. Res. 2022, 200, 1551–1560. [Google Scholar] [CrossRef] [PubMed]
- Wilbur, S.; Abadin, H.; Fay, M.; Yu, D.; Teneza, B. ATSDR D of T and HHS. Toxicological Profile for Chromium. In ATSDR’s Toxicological Profiles; CRC Press: Boca Raton, FL, USA, 2002. [Google Scholar] [CrossRef]
- Vorkamp, K.; Castaño, A.; Antignac, J.P.; Boada, L.D.; Cequier, E.; Covaci, A.; Esteban López, M.; Haug, L.S.; Kasper-Sonnenberg, M.; Koch, H.M.; et al. Biomarkers, matrices and analytical methods targeting human exposure to chemicals selected for a European human biomonitoring initiative. Environ. Int. 2021, 146, 106082. [Google Scholar] [CrossRef] [PubMed]
- Junaid, M.; Hashmi, M.Z.; Malik, R.N.; Pei, D.S. Toxicity and oxidative stress induced by chromium in workers exposed from different occupational settings around the globe: A review. Environ. Sci. Pollut. Res. 2016, 23, 20151–20167. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wise, J.T.F.; Zhang, Z.; Shi, X. Progress and Prospects of Reactive Oxygen Species in Metal Carcinogenesis. Curr. Pharmacol. Rep. 2016, 2, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Z.; Cai, T.; Li, J.; Zhang, D.; Yu, Y.; Huang, C. Hexavalent Chromium Cr(VI) Up-Regulates COX-2 Expression through an NFκB/c-Jun/AP-1–Dependent Pathway. Environ. Health Perspect. 2012, 120, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.Y.; Murphy, A.; Sun, H.; Costa, M. Molecular and epigenetic mechanisms of Cr(VI)-induced carcinogenesis. Toxicol. Appl. Pharmacol. 2019, 377, 114636. [Google Scholar] [CrossRef] [PubMed]
- Rager, J.E.; Suh, M.; Chappell, G.A.; Thompson, C.M.; Proctor, D.M. Review of transcriptomic responses to hexavalent chromium exposure in lung cells supports a role of epigenetic mediators in carcinogenesis. Toxicol. Lett. 2019, 305, 40–50. [Google Scholar] [CrossRef]
- Jia, J.; Li, T.; Yao, C.; Chen, J.; Feng, L.; Jiang, Z.; Shi, L.; Liu, J.; Chen, J.; Lou, J. Circulating differential miRNAs profiling and expression in hexavalent chromium exposed electroplating workers. Chemosphere 2020, 260, 127546. [Google Scholar] [CrossRef]
- Arakawa, H.; Weng, M.-W.; Chen, W.-C.; Tang, M.-S. Chromium (VI) induces both bulky DNA adducts and oxidative DNA damage at adenines and guanines in the p53 gene of human lung cells. Carcinogenesis 2012, 33, 1993–2000. [Google Scholar] [CrossRef]
- Wise, S.S.; Aboueissa, A.E.-M.; Martino, J.; Wise, J.P. Hexavalent Chromium–Induced Chromosome Instability Drives Permanent and Heritable Numerical and Structural Changes and a DNA Repair–Deficient Phenotype. Cancer Res. 2018, 78, 4203–4214. [Google Scholar] [CrossRef]
- Clementino, M.; Shi, X.; Zhang, Z. Oxidative stress and metabolic reprogramming in Cr(VI) carcinogenesis. Curr. Opin. Toxicol. 2018, 8, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Nickens, K.P.; Patierno, S.R.; Ceryak, S. Chromium genotoxicity: A double-edged sword. Chem. Biol. Interact. 2010, 188, 276–288. [Google Scholar] [CrossRef]
- ANSES. Valeurs Limites d’Exposition en Milieu Professionnel: Évaluation des Indicateurs Biologiques d’Exposition et Recommandation de Valeurs Biologiques pour le Chrome VI et ses Composés. 2017. Available online: https://www.anses.fr/fr/content/avis-et-rapport-de-lanses-relatif-%C3%A0-levaluation-des-indicateurs-biologiques-dexposition-et-1 (accessed on 13 July 2021).
- De Minister van Sociale Zaken en Werkgelegenheid. Regeling van de Minister van Sociale Zaken en Werkgelegenheid van 18 Oktober 2016, 2016-0000222216, tot Wijziging van de Arbeidsomstandighedenregeling in Verband de Wijziging van twee Wettelijke Grenswaarden in Bijlage XIII (Bisfenol A en Chroom (VI)-verb. 2016. Available online: https://zoek.officielebekendmakingen.nl/stcrt-2016-57792.html (accessed on 17 June 2022).
- DHI. Denmark Lowers Limit Value for Chromium VI in Work Environment. 2020. Available online: https://tox.dhi.dk/en/news/news/article/denmark-lowers-limit-value-for-chromium-vi-in-work-environment/ (accessed on 17 June 2022).
- Balachandar, V.; Arun, M.; Mohana Devi, S.; Velmurugan, P.; Manikantan, P.; Karthick Kumar, A.; Sasikala, K.; Venkatesan, C. Evaluation of the genetic alterations in direct and indirect exposures of hexavalent chromium [Cr(VI)] in leather tanning industry workers North Arcot District, South India. Int. Arch. Occup. Environ. Health 2010, 83, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Santonen, T.; Alimonti, A.; Bocca, B.; Duca, R.C.; Galea, K.S.; Godderis, L.; Göen, T.; Gomes, B.; Hanser, O.; Iavicoli, I.; et al. Setting up a collaborative European human biological monitoring study on occupational exposure to hexavalent chromium. Environ. Res. 2019, 177, 108583. [Google Scholar] [CrossRef] [PubMed]
- Santonen, T.; Porras, S.P.; Bocca, B.; Bousoumah, R.; Duca, R.C.; Galea, K.S.; Godderis, L.; Göen, T.; Hardy, E.; Iavicoli, I.; et al. HBM4EU chromates study-Overall results and recommendations for the biomonitoring of occupational exposure to hexavalent chromium. Environ. Res. 2022, 204, 111984. [Google Scholar] [CrossRef]
- Verdonck, J.; Duca, R.C.; Galea, K.S.; Iavicoli, I.; Poels, K.; Töreyin, Z.N.; Vanoirbeek, J.; Godderis, L. Systematic review of biomonitoring data on occupational exposure to hexavalent chromium. Int. J. Hyg. Environ. Health 2021, 236, 113799. [Google Scholar] [CrossRef]
- Bonassi, S.; Znaor, A.; Ceppi, M.; Lando, C.; Chang, W.P.; Holland, N.; Kirsch-Volders, M.; Zeiger, E.; Ban, S.; Barale, R.; et al. An increased micronucleus frequency in peripheral blood lymphocytes predicts the risk of cancer in humans. Carcinogenesis 2007, 28, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Abramsson-Zetterberg, L.; Zetterberg, G.; Bergqvist, M.; Grawé, J. Human cytogenetic biomonitoring using flow-cytometric analysis of micronuclei in transferrin-positive immature peripheral blood reticulocytes. Environ. Mol. Mutagen. 2000, 36, 22–31. [Google Scholar] [CrossRef]
- Costa, C.; Silva, S.; Neves, J.; Coelho, P.; Costa, S.; Laffon, B.; Snawder, J.; Teixeira, J.P. Micronucleus Frequencies in Lymphocytes and Reticulocytes in a Pesticide-Exposed Population in Portugal. J. Toxicol. Environ. Health Part A 2011, 74, 960–970. [Google Scholar] [CrossRef]
- Font-Ribera, L.; Marco, E.; Grimalt, J.O.; Pastor, S.; Marcos, R.; Abramsson-Zetterberg, L.; Pedersen, M.; Grummt, T.; Junek, R.; Barreiro, E.; et al. Exposure to disinfection by-products in swimming pools and biomarkers of genotoxicity and respiratory damage—The PISCINA2 Study. Environ. Int. 2019, 131, 104988. [Google Scholar] [CrossRef]
- Montero-Montoya, R.D.; López-Vargas, R.; Méndez-Serrano, A.; Galicia-Alonso, I.; García-Vargas, G.; Serrano-García, L.; Beltrán-Portugal, R.; Rosado-Zaidi, S.; Albores-Medina, A.; Oropeza-Hernández, L.; et al. Increased micronucleus frequencies in reticulocytes of children exposed to industrial pollution: Oxidative stress and the OGG1 S326C polymorphism. Mutat. Res. Toxicol. Environ. Mutagen. 2020, 853, 503170. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.H.G.; Saber, A.T.; Frederiksen, M.; Clausen, P.A.; Sejbaek, C.S.; Hemmingsen, C.H.; Ebbehøj, N.E.; Catalán, J.; Aimonen, K.; Koivisto, J.; et al. Occupational exposure and markers of genetic damage, systemic inflammation and lung function: A Danish cross-sectional study among air force personnel. Sci. Rep. 2021, 11, 17998. [Google Scholar] [CrossRef] [PubMed]
- Stopper, H.; Hempel, K.; Reiners, C.; Vershenya, S.; Lorenz, R.; Vukicevic, V.; Heidland, A.; Grawe, J. Pilot study for comparison of reticulocyte-micronulei with lymphocyte-micronuclei in human biomonitoring. Toxicol. Lett. 2005, 156, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Tice, R.R.; Agurell, E.; Anderson, D.; Burlinson, B.; Hartmann, A.; Kobayashi, H.; Miyamae, Y.; Rojas, E.; Ryu, J.C.; Sasaki, Y.F. Single cell gel/comet assay: Guidelines for in vitro and in vivo genetic toxicology testing. Environ. Mol. Mutagen. 2000, 35, 206–221. [Google Scholar] [CrossRef]
- Milić, M.; Ceppi, M.; Bruzzone, M.; Azqueta, A.; Brunborg, G.; Godschalk, R.; Koppen, G.; Langie, S.; Møller, P.; Teixeira, J.P.; et al. The hCOMET project: International database comparison of results with the comet assay in human biomonitoring. Baseline frequency of DNA damage and effect of main confounders. Mutat. Res. Mutat. Res. 2021, 787, 108371. [Google Scholar] [CrossRef]
- Møller, P.; Knudsen, L.E.; Loft, S.; Wallin, H. The comet assay as a rapid test in biomonitoring occupational exposure to DNA-damaging agents and effect of confounding factors. Cancer Epidemiol. Biomark. Prev. 2000, 9, 1005–1015. [Google Scholar]
- Benova, D.; Hadjidekova, V.; Hristova, R.; Nikolova, T.; Boulanova, M.; Georgieva, I.; Grigorova, M.; Popov, T.; Panev, T.; Georgieva, R.; et al. Cytogenetic effects of hexavalent chromium in Bulgarian chromium platers. Mutat. Res.-Genet. Toxicol. Environ. Mutagen. 2002, 514, 29–38. [Google Scholar] [CrossRef]
- Li, P.; Li, Y.; Zhang, J.; Yu, S.-F.; Wang, Z.-L.; Jia, G. Establishment of a reference value for chromium in the blood for biological monitoring among occupational chromium workers. Toxicol. Ind. Health 2016, 32, 1737–1744. [Google Scholar] [CrossRef]
- Sudha, S.; Kripa, S.K.; Shibily, P.; Shyn, J. Elevated frequencies of micronuclei and other nuclear abnormalities of chrome plating workers occupationally exposed to hexavalent chromium. Iran. J. Cancer Prev. 2011, 4, 120–125. [Google Scholar]
- Sudha, S.; Prathyumnan, S.; Keyan, K.S.; Joseph, S.; Vasudevan, B.S.G.; Sasikala, K. Evaluation of DNA damage induction and repair inhibition in welders exposed to hexavalent chromium. Asian Pac. J. Cancer Prev. 2010, 11, 95–100. [Google Scholar]
- Muller, C.D.; Garcia, S.C.; Brucker, N.; Goethel, G.; Sauer, E.; Lacerda, L.M.; Oliveira, E.; Trombini, T.L.; Machado, A.B.; Pressotto, A.; et al. Occupational risk assessment of exposure to metals in chrome plating workers. Drug Chem. Toxicol. 2022, 45, 560–567. [Google Scholar] [CrossRef]
- Ambreen, K.; Khan, F.H.; Bhadauria, S.; Kumar, S. Genotoxicity and oxidative stress in chromium-exposed tannery workers in North India. Toxicol. Ind. Health 2014, 30, 405–414. [Google Scholar] [CrossRef]
- Li, P.; Gu, Y.; Yu, S.; Li, Y.; Yang, J.; Jia, G. Assessing the suitability of 8OHdG and micronuclei as genotoxic biomarkers in chromateexposed workers: A crosssectional study. BMJ Open 2014, 4, e005979. [Google Scholar] [CrossRef] [PubMed]
- Ndaw, S.; Leso, V.; Bousoumah, R.; Rémy, A.; Bocca, B.; Duca, R.C.; Godderis, L.; Hardy, E.; Janasik, B.; van Nieuwenhuyse, A.; et al. HBM4EU chromates study-Usefulness of measurement of blood chromium levels in the assessment of occupational Cr(VI) exposure. Environ. Res. 2022, 214, 113758. [Google Scholar] [CrossRef]
- Nübler, S.; Schäfer, M.; Haji-Abbas-Zarrabi, K.; Marković, S.; Marković, K.; Esteban López, M.; Castaño, A.; Mol, H.; Koch, H.M.; Antignac, J.-P.; et al. Interlaboratory Comparison Investigations (ICIs) for human biomonitoring of chromium as part of the quality assurance programme under HBM4EU. J. Trace Elem. Med. Biol. 2022, 70, 126912. [Google Scholar] [CrossRef] [PubMed]
- Esteban López, M.; Göen, T.; Mol, H.; Nübler, S.; Haji-Abbas-Zarrabi, K.; Koch, H.M.; Kasper-Sonnenberg, M.; Dvorakova, D.; Hajslova, J.; Antignac, J.-P.; et al. The European human biomonitoring platform-Design and implementation of a laboratory quality assurance/quality control (QA/QC) programme for selected priority chemicals. Int. J. Hyg. Environ. Health 2021, 234, 113740. [Google Scholar] [CrossRef] [PubMed]
- Vital, N.; Antunes, S.; Louro, H.; Vaz, F.; Simões, T.; Penque, D.; Silva, M.J. Environmental Tobacco Smoke in Occupational Settings: Effect and Susceptibility Biomarkers in Workers From Lisbon Restaurants and Bars. Front. Public Health 2021, 9, 700. [Google Scholar] [CrossRef]
- Fenech, M.; Chang, W.; Kirsch-Volders, M.; Holland, N.; Bonassi, S.; Zeiger, E. HUMN project: Detailed description of the scoring criteria for the cytokinesis-block micronucleus assay using isolated human lymphocyte cultures. Mutat. Res. Toxicol. Environ. Mutagen. 2003, 534, 65–75. [Google Scholar] [CrossRef]
- Fenech, M. Cytokinesis-block micronucleus cytome assay. Nat. Protoc. 2007, 2, 1084–1104. [Google Scholar] [CrossRef]
- OECD. Test 487: In Vitro Mammalian Cell Micronucleus Test. In OECD Guidelines for the Testing of Chemicals, Section 4; OECD: Paris, France, 2016; pp. 1–29. [Google Scholar] [CrossRef]
- Collins, A.R. Measuring oxidative damage to DNA and its repair with the comet assay. Biochim. Et Biophys. Acta-Gen. Subj. 2014, 2, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Hosozumi, C.; Toriba, A.; Chuesaard, T.; Kameda, T.; Tang, N.; Hayakawa, K. Analysis of 8-hydroxy-2’-deoxyguanosine in human urine using hydrophilic interaction chromatography with tandem mass spectrometry. J. Chromatogr. B 2012, 893, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-L.; Huang, Y.-J.; Pan, C.-H.; Hu, C.-W.; Chao, M.-R. Determination of urinary malondialdehyde by isotope dilution LC-MS/MS with automated solid-phase extraction: A cautionary note on derivatization optimization. Free Radic. Biol. Med. 2011, 51, 1823–1829. [Google Scholar] [CrossRef] [PubMed]
- Domingo, J.L.; Perelló, G.; Giné Bordonaba, J. Dietary Intake of Metals by the Population of Tarragona County (Catalonia, Spain): Results from a Duplicate Diet Study. Biol. Trace Elem. Res. 2012, 146, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.; Pina, C.; Coelho, P.; Costa, C.; Silva, S.; Porto, B.; Laffon, B.; Teixeira, J.P. Occupational Exposure to Formaldehyde: Genotoxic Risk Evaluation By Comet Assay And Micronucleus Test Using Human Peripheral Lymphocytes. J. Toxicol. Environ. Health Part A 2011, 74, 1040–1051. [Google Scholar] [CrossRef] [PubMed]
- Fenech, M.; Holland, N.; Zeiger, E.; Chang, W.P.; Burgaz, S.; Thomas, P.; Bolognesi, C.; Knasmueller, S.; Kirsch-Volders, M.; Bonassi, S. The HUMN and HUMNxL international collaboration projects on human micronucleus assays in lymphocytes and buccal cells—Past, present and future. Mutagenesis 2011, 26, 239–245. [Google Scholar] [CrossRef]
- Murgia, E.; Ballardin, M.; Bonassi, S.; Rossi, A.M.; Barale, R. Validation of micronuclei frequency in peripheral blood lymphocytes as early cancer risk biomarker in a nested case–control study. Mutat. Res. Mol. Mech. Mutagen. 2008, 639, 27–34. [Google Scholar] [CrossRef]
- Ray, R.R. Adverse hematological effects of hexavalent chromium: An overview. Interdiscip. Toxicol. 2016, 9, 55–65. [Google Scholar] [CrossRef]
- Xiaohua, L.; Yanshuang, S.; Li, W.; Yuhui, L.; Ji, Z.; Yanhui, M.; Yun, W.; Wenjun, M.; Lei, Y.; Guang, J. Evaluation of the Correlation Between Genetic Damage and Occupational Chromate Exposure Through BNMN Frequencies. J. Occup. Environ. Med. 2012, 54, 166–170. [Google Scholar] [CrossRef]
- Li, Y.; Hu, G.; Li, P.; Tang, S.; Zhang, J.; Jia, G. miR-3940-5p enhances homologous recombination after DSB in Cr(VI) exposed 16HBE cell. Toxicology 2016, 344, 1–6. [Google Scholar] [CrossRef]
- Wang, T.-C.; Song, Y.-S.; Wang, H.; Zhang, J.; Yu, S.-F.; Gu, Y.-E.; Chen, T.; Wang, Y.; Shen, H.-Q.; Jia, G. Oxidative DNA damage and global DNA hypomethylation are related to folate deficiency in chromate manufacturing workers. J. Hazard. Mater. 2012, 213, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Huvinen, M.; Mäkitie, A.; Järventaus, H.; Wolff, H.; Stjernvall, T.; Hovi, A.; Hirvonen, A.; Ranta, R.; Nurminen, M.; Norppa, H. Nasal cell micronuclei, cytology and clinical symptoms in stainless steel production workers exposed to chromium. Mutagenesis 2002, 17, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Maeng, S.H.; Chung, H.W.; Kim, K.J.; Lee, B.M.; Shin, Y.C.; Kim, S.J.; Yu, I.J. Chromosome aberration and lipid peroxidation in chromium-exposed workers. Biomarkers 2004, 9, 418–434. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-H.; Zhang, X.; Wang, X.-C.; Jin, L.-F.; Yang, Z.-P.; Jiang, C.-X.; Chen, Q.; Ren, X.-B.; Cao, J.-Z.; Wang, Q.; et al. Chronic occupational exposure to hexavalent chromium causes DNA damage in electroplating workers. BMC Public Health 2011, 11, 224. [Google Scholar] [CrossRef] [PubMed]
- Viegas, S.; Martins, C.; Bocca, B.; Bousoumah, R.; Duca, R.C.; Galea, K.S.; Godderis, L.; Iavicoli, I.; Janasik, B.; Jones, K.; et al. HBM4EU Chromates Study: Determinants of Exposure to Hexavalent Chromium in Plating, Welding and Other Occupational Settings. Int. J. Environ. Res. Public Health 2022, 19, 3683. [Google Scholar] [CrossRef] [PubMed]
- Azqueta, A.; Ladeira, C.; Giovannelli, L.; Boutet-Robinet, E.; Bonassi, S.; Neri, M.; Gajski, G.; Duthie, S.; Del Bo’, C.; Riso, P.; et al. Application of the comet assay in human biomonitoring: An hCOMET perspective. Mutat. Res. Mutat. Res. 2020, 783, 108288. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Izakovic, M.; Mazur, M.; Rhodes, C.J.; Telser, J. Role of oxygen radicals in DNA damage and cancer incidence. Mol. Cell Biochem. 2004, 266, 37–56. [Google Scholar] [CrossRef]
- Andreoli, R.; Mutti, A.; Goldoni, M.; Manini, P.; Apostoli, P.; De Palma, G. Reference ranges of urinary biomarkers of oxidized guanine in (2’-deoxy)ribonucleotides and nucleic acids. Free Radic. Biol. Med. 2011, 50, 254–261. [Google Scholar] [CrossRef]
- Tranfo, G.; Paci, E.; Carrieri, M.; Marchetti, E.; Sisto, R.; Gherardi, M.; Costabile, F.; Bauleo, L.; Ancona, C.; Pigini, D. Levels of Urinary Biomarkers of Oxidatively Generated Damage to DNA and RNA in Different Groups of Workers Compared to General Population. Int. J. Environ. Res. Public Health 2019, 16, 2995. [Google Scholar] [CrossRef]
- Lindberg, E.; Vesterberg, O. Urinary excretion of chromium in chromeplaters after discontinued exposure. Am. J. Ind. Med. 1989, 16, 485–492. [Google Scholar] [CrossRef]
- Pan, C.-H.; Jeng, H.A.; Lai, C.-H. Biomarkers of oxidative stress in electroplating workers exposed to hexavalent chromium. J. Expo. Sci. Environ. Epidemiol. 2018, 28, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Zendehdel, R.; Shetab-Boushehri, S.V.; Azari, M.R.; Hosseini, V.; Mohammadi, H. Chemometrics models for assessment of oxidative stress risk in chrome-electroplating workers. Drug Chem. Toxicol. 2015, 38, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Maeng, S.-H.; Chung, H.-W.; Yu, I.-J.; Kim, H.-Y.; Lim, C.-H.; Kim, K.-J.; Ootsuyama, Y.; Kasai, H. Changes of 8-OH-dG levels in DNA and its base excision repair activity in rat lungs after inhalation exposure to hexavalent chromium. Mutat. Res. Toxicol. Environ. Mutagen. 2003, 539, 109–116. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Independent Variables | Participants with MN PBL Data n (%) | Participants with MN RET Data n (%) | Participants with Comet Assay Data n (%) | Participants with Oxidative stress Biomarkers Data n (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Participants | Total Workers | Total Controls a | Total Participants | Total Workers | Total Controls a | Total Participants | Total Workers | Total Controls a | Total Participants | Total Workers | Total Controls a | |
| n | 284 | 191 (67.3) | 93 (32.7) | 256 | 170 (66.4) | 86 (33.6) | 117 | 74 (63.2) | 43 (36.8) | 299 | 215 (71.9) | 84 (28.1) |
| Country | 284 | 256 | 117 | 299 | ||||||||
| Belgium | 69 (24.3) | 48 (25.1) | 21 (22.6) | 69 (27.0) | 48 (28.2) | 21 (24.4) | 29 (24.8) | 16 (21.6) | 13 (30.2) | 67 (22.4) | 53 (24.7) | 14 (16.7) |
| Finland | 56 (19.7) | 33 (17.3) | 23 (24.7) | 61 (23.8) | 37 (21.8) | 24 (27.9) | 20 (17.1) | 14 (18.9) | 6 (14.0) | 72 (24.1) | 47 (21.9) | 25 (29.8) |
| Netherlands | 30 (10.6) | 20 (10.5) | 10 (10.8) | 30 (10.0) | 20 (9.3) | 10 (11.9) | ||||||
| Poland | 71 (25.0) | 52 (27.2) | 19 (20.4) | 69 (27.0) | 51 (30.0) | 18 (20.9) | 8 (6.8) | 5 (6.8) | 3 (7.0) | 71 (23.7) | 52 (24.2) | 19 (22.6) |
| Portugal | 58 (20.4) | 38 (19.9) | 20 (21.5) | 57 (22.3) | 34 (20.0) | 23 (26.7) | 60 (51.3) | 39 (52.7) | 21 (48.8) | |||
| France | 59 (19.7) | 43 (20.0) | 16 (19.0) | |||||||||
| Sex | 284 | 256 | 117 | 299 | ||||||||
| Female | 35 (12.3) | 7 (3.7) | 28 (30.1) | 30 (11.7) | 7 (4.1) | 23 (26.7) | 15 (12.8) | 5 (6.8) | 10 (23.3) | 32 (10.7) | 4 (1.9) | 28 (33.3) |
| Male | 249 (87.7) | 184 (96.3) | 65 (69.9) | 226 (88.3) | 163 (95.9) | 63 (73.3) | 102 (87.2) | 69 (93.2) | 33 (76.7) | 267 (89.3) | 211 (98.1) | 56 (66.7) |
| Age | ||||||||||||
| Mean | 42.0 | 41.1 | 43.6 | 41.9 | 41.1 | 43.5 | 43.5 | 42.8 | 44.6 | 41.7 | 41.1 | 43.4 |
| SD | 10.4 | 11.0 | 8.88 | 10.5 | 11.1 | 9.28 | 9.94 | 11.0 | 7.89 | 10.5 | 10.6 | 9.88 |
| Min–max | 20–68 | 20–68 | 23–63 | 20–68 | 20–68 | 23–63 | 20–64 | 20–64 | 30–60 | 20–68 | 20–68 | 23–63 |
| Age group | 274 | 246 | 110 | 293 | ||||||||
| 20–49 | 200 (73.0) | 132 (72.5) | 68 (73.9) | 179 (72.8) | 116 (72.0) | 63 (74.1) | 76 (69.1) | 47 (69.1) | 29 (69.0) | 217 (74.1) | 154 (73.3) | 63 (75.9) |
| 50–68 | 74 (27.0) | 50 (27.5) | 24 (26.1) | 67 (27.2) | 45 (28.0) | 22 (25.9) | 34 (30.9) | 21 (30.9) | 13 (31.0) | 76 (25.9) | 56 (26.7) | 20 (24.1) |
| Smoking | 279 | 251 | 112 | 296 | ||||||||
| Smoker | 78 (28.0) | 69 (36.9) | 12 (13.0) | 66 (26.3) | 55 (33.1) | 11 (12.9) | 29 (25.9) | 22 (31.4) | 7 (16.7) | 81 (27.4) | 72 (33.8) | 9 (10.8) |
| Former smoker | 35 (12.5) | 46 (24.6) | 13 (14.1) | 52 (20.7) | 41 (24.7) | 11 (12.9) | 24 (21.4) | 18 (25.7) | 6 (14.3) | 73 (24.7) | 59 (27.7) | 14 (16.9) |
| Non smoker | 166 (59.5) | 72 (38.5) | 67 (72.8) | 133 (53.0) | 70 (42.2) | 63 (74.1) | 59 (52.7) | 30 (42.9) | 29 (69.0) | 142 (48.0) | 82 (38.5) | 60 (72.3) |
| Alcohol | 279 | 251 | 112 | 296 | ||||||||
| No | 51 (18.3) | 34 (18.2) | 17 (18.5) | 45 (17.9) | 29 (17.5) | 16 (18.8) | 30 (26.8) | 21 (30.0) | 9 (21.4) | 40 (13.5) | 29 (13.6) | 11 (13.3) |
| Low | 114 (40.9) | 79 (42.2) | 35 (38.0) | 116 (46.2) | 79 (47.6) | 37 (43.5) | 30 (26.8) | 13 (18.6) | 17 (40.5) | 128 (43.2) | 94 (44.1) | 34 (41.0) |
| High | 114 (40.9) | 74 (36.9) | 40 (43.5) | 90 (35.9) | 58 (34.9) | 32 (37.6) | 52 (46.4) | 36 (51.4) | 16 (38.1) | 128 (43.2) | 90 (42.3) | 38 (45.8) |
| Home location | 279 | 251 | 112 | 293 | ||||||||
| Urban | 199 (71.3) | 130 (69.5) | 69 (75.0) | 175 (69.7) | 113 (68.1) | 62 (72.9) | 84 (75.0) | 55 (78.6) | 29 (69.0) | 187 (63.8) | 127 (60.2) | 60 (73.2) |
| Rural | 80 (28.7) | 57 (30.5) | 23 (25.0) | 76 (30.3) | 53 (31.9) | 23 (27.1) | 28 (25.0) | 15 (21.4) | 13 (31.0) | 106 (36.2) | 84 (39.8) | 22 (26.8) |
| Industrial area | 275 | 247 | 112 | 294 | ||||||||
| No | 206 (74.9) | 134 (73.2) | 72 (78.3) | 183 (74.1) | 116 (71.6) | 67 (78.8) | 89 (79.5) | 54 (77.1) | 35 (83.3) | 207 (70.4) | 152 (72.0) | 55 (66.3) |
| Yes | 69 (25.1) | 49 (26.8) | 20 (21.7) | 64 (25.9) | 46 (28.4) | 18 (21.2) | 23 (20.5) | 16 (22.9) | 7 (16.7) | 87 (29.6) | 59 (28.0) | 28 (33.7) |
| Traffic density | 279 | 251 | 109 | 296 | ||||||||
| Low | 139 (49.8) | 96 (51.3) | 43 (46.7) | 119 (47.4) | 82 (49.4) | 37 (43.5) | 59 (52.7) | 37 (52.9) | 22 (52.4) | 160 (54.1) | 119 (55.9) | 41 (49.4) |
| Medium | 113 (40.5) | 70 (37.4) | 43 (46.7) | 108 (43.0) | 66 (39.8) | 42 (49.4) | 42 (37.5) | 25 (35.7) | 17 (40.5) | 103 (34.8) | 68 (31.9) | 35 (42.2) |
| Heavy | 27 (9.7) | 21 (11.2) | 6 (6.5) | 24 (9.6) | 18 (10.8) | 6 (7.1) | 11 (9.8) | 8 (11.4) | 3 (7.1) | 33 (11.1) | 26 (12.2) | 7 (8.4) |
| MN PBL | MN RET | Comet Assay | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | MNBC (‰) | MN in BC (‰) | NPB (‰) | NBUD (‰) | CBPI | n | Micronucleated +CD71 Reticulocytes (‰) | n | Tail Intensity (%) | |
| Total exposed Group | 191 | 9.11 ± 6.08 * £ | 10.47 ± 7.19 * £ | 1.76 ± 2.92 £ | 0.57 ± 0.97 * | 1.85 ± 0.26 * £ | 170 | 2.75 ± 1.92 £ | 74 | 6.34 ± 1.83 * £ ¥ |
| Bath plating workers | 39 | 12.56 ± 8.04 £ | 14.32 ± 9.64 £ | 3.02 ± 3.56 £ | 0.65 ± 0.98 £ | 1.72 ± 0.33 * | 19 | 1.88 ± 1.14 * | 12 | 7.36 ± 1.61 £ ¥ |
| Chromate paint applicators | 34 | 9.72 ± 6.36 £ | 10.82 ± 7.07 £ | 1.65 ± 2.98 | 0.40 ± 0.74 * ¥ | 1.83 ± 0.24 | 33 | 2.03 ± 1.11 * | 25 | 5.24 ± 1.26 * £ |
| Welders | 87 | 7.37 ± 4.78 * ¥ | 8.55 ± 5.79 * ¥ | 1.51 ± 2.89 £ | 0.60 ± 1.08 * | 1.86 ± 0.23 £ | 90 | 3.40 ± 2.25 £ ¥ | 19 | 7.62 ± 1.92 £ ¥ |
| Machining workers | 12 | 8.04 ± 3.09 | 9.62 ± 4.01 | 0.63 ± 0.91 £ | 0.79 ± 0.99 * ¥ | 2.00 ± 0.23 £ | 10 | 2.30 ± 1.34 | 5 | 5.04 ± 2.03 £ |
| Other activities | 19 | 9.60 ± 4.76 £ | 11.27 ± 5.97 £ | 1.17 ± 1.21 | 0.39 ± 0.74 | 1.98 ± 0.14 £ | 18 | 1.97 ± 0.72 | 13 | 6.12 ± 1.04 * £ |
| Total control Group | 93 | 10.47 ± 7.26 | 11.88 ± 8.19 | 1.77 ± 2.36 | 0.48 ± 0.88 | 1.83 ± 0.29 | 86 | 2.62 ± 2.16 | 43 | 4.59 ± 3.26 |
| Within company | 60 | 12.19 ± 7.58 £ | 13.68 ± 8.40 £ | 2.03 ± 2.36 £ | 0.65 ± 0.97 £ | 1.88 ± 0.30 £ | 50 | 3.13 ± 2.67 £ | 24 | 6.88 ± 2.44 £ |
| Outwith company | 33 | 7.33 ± 5.47 * | 8.61 ± 6.77* | 1.29 ± 2.30 * | 0.18 ± 0.41 * | 1.74 ± 0.24 * | 36 | 1.92 ± 0.68 * | 19 | 1.71 ± 1.18 * |
| MN PBL | MN RET | Comet—Tail Intensity | MDA Pre-Shift | MDA Post-Shift | 8-OHdG Pre-Shift | 8-OHdG Post-Shift | ||
|---|---|---|---|---|---|---|---|---|
| MN PBL | n | 247 | 114 | 307 | 162 | 207 | 162 | |
| Corr. Coef | −0.143 | 0.440 | 0.042 | 0.070 | 0.090 | 0.022 | ||
| p | 0.024 | <0.001 | 0.547 | 0.376 | 0.197 | 0.786 | ||
| MN RET | n | 112 | 182 | 137 | 182 | 137 | ||
| Corr. Coef | 0.078 | −0.020 | 0.080 | −0.069 | 0.096 | |||
| p | 0.414 | 0.788 | 0.353 | 0.358 | 0.264 | |||
| Comet—tail intensity | n | 44 | 36 | 44 | 36 | |||
| Corr. Coef | −0.105 | −0.025 | −0.058 | 0.077 | ||||
| p | 0.499 | 0.885 | 0.710 | 0.653 | ||||
| MDA pre-shift | n | 228 | 298 | 228 | ||||
| Corr. Coef | 0.277 | 0.585 | 0.114 | |||||
| p | <0.001 | <0.001 | 0.086 | |||||
| MDA post-shift | n | 228 | 229 | |||||
| Corr. Coef | 0.204 | 0.529 | ||||||
| p | 0.002 | <0.001 | ||||||
| 8-OHdG pre-shift | n | 228 | ||||||
| Corr. Coef | 0.335 | |||||||
| p | <0.001 | |||||||
| 8-OHdG post-shift | n | |||||||
| Corr. Coef | ||||||||
| p |
| MN PBL | MN RET | Comet—Tail Intensity | MDA Pre-Shift | MDA Post-Shift | 8-OHdG Pre-Shift | 8-OHdG Post-Shift | ||
|---|---|---|---|---|---|---|---|---|
| Cr in plasma | n | 279 | 251 | 112 | 284 | 217 | 284 | 217 |
| Corr. Coef | 0.361 | −0.038 | 0.476 | 0.068 | −0.115 | −0.033 | −0.099 | |
| p | <0.001 | 0.552 | <0.001 | 0.256 | 0.091 | 0.576 | 0.147 | |
| Cr in red blood cells | n | 279 | 251 | 112 | 284 | 217 | 284 | 217 |
| Corr. Coef | 0.086 | −0.098 | −0.216 | 0.027 | −0.020 | −0.126 | −0.063 | |
| p | 0.153 | 0.122 | 0.022 | 0.653 | 0.771 | 0.035 | 0.357 | |
| U-Cr (pre-shift) | n | 260 | 233 | 100 | 283 | 219 | 283 | 219 |
| Corr. Coef | 0.175 | 0.023 | 0.303 | 0.029 | −0.074 | 0.067 | −0.008 | |
| p | 0.005 | 0.723 | 0.002 | 0.626 | 0.273 | 0.258 | 0.910 | |
| U-Cr (post-shift) | n | 252 | 224 | 98 | 277 | 216 | 277 | 216 |
| Corr. Coef | 0.207 | −0.009 | 0.371 | 0.079 | −0.207 | 0.072 | −0.162 | |
| p | 0.001 | 0.888 | <0.001 | 0.190 | 0.002 | 0.234 | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavares, A.; Aimonen, K.; Ndaw, S.; Fučić, A.; Catalán, J.; Duca, R.C.; Godderis, L.; Gomes, B.C.; Janasik, B.; Ladeira, C.; et al. HBM4EU Chromates Study—Genotoxicity and Oxidative Stress Biomarkers in Workers Exposed to Hexavalent Chromium. Toxics 2022, 10, 483. https://doi.org/10.3390/toxics10080483
Tavares A, Aimonen K, Ndaw S, Fučić A, Catalán J, Duca RC, Godderis L, Gomes BC, Janasik B, Ladeira C, et al. HBM4EU Chromates Study—Genotoxicity and Oxidative Stress Biomarkers in Workers Exposed to Hexavalent Chromium. Toxics. 2022; 10(8):483. https://doi.org/10.3390/toxics10080483
Chicago/Turabian StyleTavares, Ana, Kukka Aimonen, Sophie Ndaw, Aleksandra Fučić, Julia Catalán, Radu Corneliu Duca, Lode Godderis, Bruno C. Gomes, Beata Janasik, Carina Ladeira, and et al. 2022. "HBM4EU Chromates Study—Genotoxicity and Oxidative Stress Biomarkers in Workers Exposed to Hexavalent Chromium" Toxics 10, no. 8: 483. https://doi.org/10.3390/toxics10080483